

Late life depression refers to a major depressive episode occurring for the first time in an older person (usually over 50 or 60 years of age). Concurrent medical problems and lower functional expectations of elderly patients often obscure the degree of impairment. Typically, elderly patients with depression do not report depressed mood, but instead present with less specific symptoms such as insomnia, anorexia, and fatigue. Elderly persons sometimes dismiss less severe depression as an acceptable response to life stress or a normal part of aging.

Maps, Directions, and Place Reviews
Epidemiology of late life depression
Major depression of late life
Major Depression is a mental disorder characterized by an all-encompassing low mood accompanied by low self-esteem, and loss of interest or pleasure in normally enjoyable activities.Nearly 5 million of the 31 million Americans who are 65 years or older are clinically depressed, and 1 million have major depression. Approximately 3 percent of healthy elderly persons living in the community have major depression. Recurrence may be as high as 40 percent. Suicide rates are nearly twice as high in depressed patients as in the general population. Major depression is more common in medically ill patients who are older than 70 years and hospitalized or institutionalized. Severe or chronic diseases associated with high rates of depression include stroke (30 to 60 percent), coronary heart disease (8 to 44 percent), cancer (1 to 40 percent), Parkinson's disease (40 percent), Alzheimer's disease (20 to 40 percent), and dementia (17 to 31 percent).
Minor depression of late life
Minor depression is a clinically significant depressive disorder that does not fulfill the duration criterion or the number of symptoms necessary for the diagnosis of major depression. Minor depression, which is more common than major depression in elderly patients, may follow a major depressive episode. It also can be a reaction to routine stressors in older populations. Fifteen to 50 percent of patients with minor depression develop major depression within two years.
Hormone Depression Video
Symptoms and diagnosis of late life depression
To meet criteria for a major depressive episode, a patient must have 5 of these 9 symptoms nearly every day for at least 2 weeks.
- Depressed or sad mood
- Anhedonia (loss of interest in pleasurable activities)
- Sleep disturbance (increased or decreased sleep)
- Appetite disturbance (increased or decreased appetite) typically with weight change
- Energy disturbance (increased or decreased energy/activity level), usually fatigue
- Poor memory and/or concentration
- Feelings of guilt or worthlessness
- Psychomotor retardation or agitation (a change in mental and physical speed perceived by other people)
- Thoughts of wishing you were dead; suicidal ideation or suicide attempts

Causes
The exact changes in brain chemistry and function that cause either late life or earlier-onset depression are unknown. It is known, however, that brain changes can be triggered by the stresses of certain life events such as illness, childbirth, death of a loved one, life transitions (such as retirement), interpersonal conflicts, or social isolation. Risk factors for depression in elderly persons include a history of depression, chronic medical illness, female sex, being single or divorced, brain disease, alcohol abuse, use of certain medications, and stressful life events.

Treatments
Treatment is effective in about 80% of identified cases, when treatment is provided. Effective management requires a biopsychosocial approach, combining pharmacotherapy and psychotherapy. Therapy generally results in improved quality of life, enhanced functional capacity, possible improvement in medical health status, increased longevity, and lower health care costs. Improvement should be evident as early as two weeks after the start of therapy, but full therapeutic effects may require several months of treatment. Psychotherapy and medication are the two primary treatment approaches.Therapy for older patients should be continued for longer periods than are typically used in younger patients.
Psychotherapy
Psychologic therapies are recommended for elderly patients with depression because of this group's vulnerability to adverse effects and high rates of medical problems and medication use. Psychotherapeutic approaches include cognitive behavioral therapy, supportive psychotherapy, problem-solving therapy, and interpersonal therapy. The potential benefit of psychotherapy is not diminished by increasing age. Older adults often have better treatment compliance, lower dropout rates, and more positive responses to psychotherapy than younger patients. Consultation with a clinical geropsychologist is useful.
Pharmacotherapy
Pharmacotherapy for acute episodes of depression usually is effective and free of complications. Underuse or misuse of antidepressants and prescribing inadequate dosages are the most common mistakes physicians make when treating elderly patients for depression. Only 10 to 40 percent of depressed elderly patients are given medication. Antidepressants, in general, may also work by playing a neuroprotective role in how they relieve anxiety and depression. It's thought that antidepressants may increase the effects of brain receptors that help nerve cells keep sensitivity to glutamate which is an organic compound of a nonessential amino acid. This increased support of nerve cells lowers glutamate sensitivity, providing protection against the glutamate overwhelming and exciting key brain areas related to depression. Antidepressant medications are often the first treatment choice for adults with moderate or severe depression, sometimes along with psychotherapy. Although antidepressants may not cure depression, they can lead to remission, which is the disappearance or nearly complete reduction of depression symptoms.
Selective Serotonin Reuptake Inhibitors
Selective serotonin reuptake inhibitors (SSRIs) are a popular class of antidepressant medications. The first drug in this class was fluoxetine (Prozac), which hit the U.S. market in 1987. Precisely how SSRIs affect depression isn't clear. Certain brain chemicals called neurotransmitters are associated with depression, including the neurotransmitter serotonin (ser-oh-TOE-nin). Some research suggests that abnormalities in neurotransmitter activity affect mood and behavior. SSRIs seem to relieve symptoms of depression by blocking the reabsorption (reuptake) of serotonin by certain nerve cells in the brain. This leaves more serotonin available in the brain. Increased serotonin enhances neurotransmission, the sending of nerve impulses, and improves mood. SSRIs are called selective because they seem to affect only serotonin, not other neurotransmitters.
Tricyclic Antidepressants
Tricyclic antidepressants (TCAs) are a class of psychoactive drugs used primarily as antidepressants, which were first discovered in the early 1950s, and subsequently introduced later in the decade. They are named after their chemical structure, which contains three rings of atoms, and are closely related to the tetracyclic antidepressants (TeCAs), which contain four rings of atoms.
Monoamine Oxidase Inhibitors (MAOIs)
Researchers believe MAOIs relieve depression by preventing the enzyme monoamine oxidase from metabolizing the neurotransmitters norepinephrine (nor-ep-ih-NEF-rin), serotonin (ser-oh-TOE-nin) and dopamine (DOE-puh-mene) in the brain. As a result, these levels remain high in the brain, boosting mood.
Other Antidepressants
Other antidepressants exist that have different ways of working than the SSRIs, tricyclics, and MAOIs. Commonly used ones are venlafaxine, nefazadone, bupropion, mirtazapine and trazodone.
Electroconvulsive Therapy (ECT)
Electroconvulsive therapy (ECT) is a first-line option in patients with depression and psychotic features who have not responded to antipsychotic and antidepressant medications,and patients with severe nonpsychotic depression who have not responded to adequate trials of two antidepressants.
ECT is a procedure in which electric currents are passed through the brain, deliberately triggering a brief seizure. This seizure releases many chemicals in the brain. These chemicals, called neurotransmitters, deliver messages from one brain cell to another. The release of these chemicals makes the brain cells work better. A person's mood will improve when his or her brain cells and chemical messengers work better. Although electroconvulsive therapy can still cause side effects and complications, it now uses precisely calculated electrical currents administered in a controlled setting to achieve the most benefit with the fewest possible risks.
Deep Brain Stimulation (DBS)
Deep brain stimulation (DBS) is a surgical treatment involving the implantation of a medical device called a brain pacemaker, which sends electrical impulses to specific parts of the brain. DBS in select brain regions has provided remarkable therapeutic benefits for otherwise treatment-resistant movement and affective disorders such as chronic pain, Parkinson's disease, tremor and dystonia. Despite the long history of DBS, its underlying principles and mechanisms are still not clear. DBS directly changes brain activity in a controlled manner, its effects are reversible (unlike those of lesioning techniques) and is one of only a few neurosurgical methods that allows blinded studies.
Transcranial Magnetic Stimulation (TMS)
Transcranial magnetic stimulation (TMS) is a procedure that uses magnetic fields to stimulate nerve cells in the brain to improve symptoms of depression. Transcranial magnetic stimulation is one of the newer types of brain-stimulation methods designed to treat depression when standard treatment hasn't worked. There are different ways to perform transcranial magnetic stimulation. But in general, a large electromagnetic coil is placed against the scalp near the forehead. The electromagnet creates painless electric currents that stimulate nerve cells in the region of your brain involved in mood regulation and depression.
Vagus Nerve Stimulation (VNS)
Vagus nerve stimulation (VNS) is a neurological procedure that sends electrical impulses into the brain in an effort to improve chronic depression symptoms. Vagus nerve stimulation is one of several newer types of brain stimulation methods designed to treat depression when standard treatment hasn't worked. Vagus nerve stimulation is sometimes called vagal nerve stimulation. With vagus nerve stimulation, a device called a pulse generator is surgically implanted in the chest. A wire threaded under the skin connects the pulse generator to the left vagus nerve in the neck. The pulse generator sends out electrical signals along the vagus nerve to the brain. These signals affect mood centers in the brain, possibly improving depression symptoms. Vagus nerve stimulation is recommended only for certain cases of severe or chronic depression.

Research
Genetics Research
Researchers are increasingly certain that genes play an important role in vulnerability to depression. In recent years, the search for a single, defective gene responsible for each mental illness has given way to the understanding that multiple gene variants, acting together with yet unknown environmental risk factors or developmental events, account for the expression of depression.
Brain Imaging Research
Brain imaging (functional/structural MRI) may help direct the search for microscopic abnormalities in brain structure and function responsible for late life depression. Ultimately, imaging technologies may serve as tools for early diagnosis and subtyping of depression.
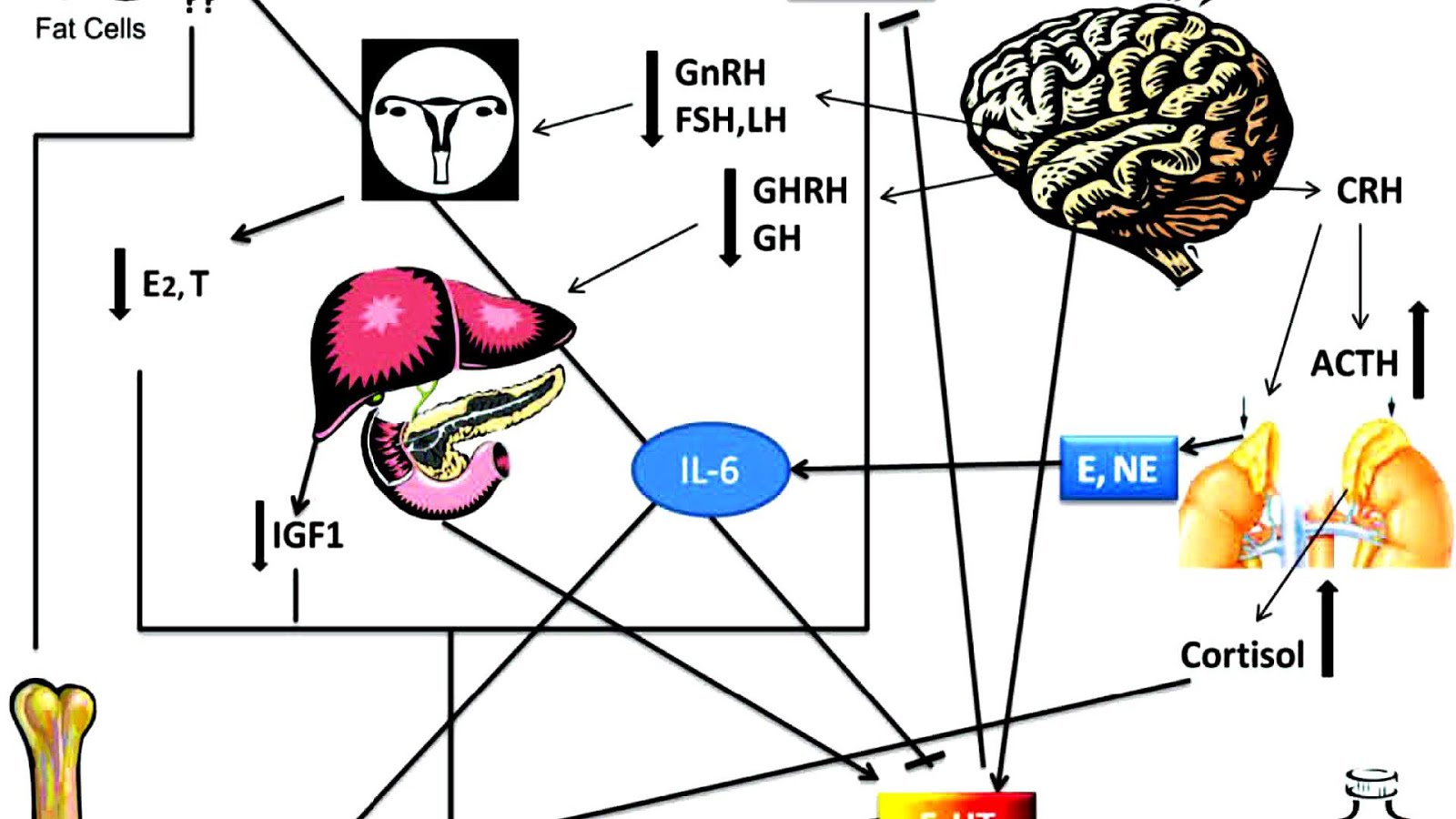
Hormonal Abnormalities Research
The hormonal system that regulates the body's response to stress, the hypothalamic-pituitary-adrenal axis (HPA), is overactive in many patients with depression. Researchers are investigating whether this phenomenon contributes to the development of depression.

Additional information
- Major Depressive Disorder
- Depression
- Clinical Geropsychology
- Deep brain stimulation
- Tricyclic antidepressant
- Monoamine oxidase inhibitor
Source of the article : Wikipedia
EmoticonEmoticon